10 Lessons Learned After a Year of COVID-19

It’s been a year of the unprecedented. City streets emptied, strong health systems faltered, and more than two million people lost their lives to COVID-19 around the world. Through these hardships we forged ahead with reimagined programs and an ever-evolving emergency response—and we’re still going.
Though it hasn’t been easy, we learned lessons every step of the way. A year into our pandemic response, and we’re sharing our top ten lessons learned so far.
1. COVID-19 is forcing the world to recognize inequalities.

COVID-19 devastated even the most well-resourced health systems around the world. Hospitals were overwhelmed; health care workers went without adequate access to PPE and patients without ventilators. The result was a soaring death toll.
Then there were countries like Peru, Kenya, South Sudan, Zambia, and Haiti—the five countries we serve and five countries whose health care systems are desperately fragile. Their capacity to respond to COVID-19 was overwhelmingly inadequate. With many facilities operating without running water, the threat was tenfold. This was the reality that drove CMMB’s rapid response in the early days of the pandemic.
2. The corollary risks of the virus proved devastating.
Many of the communities we serve know what it’s like to live through a public health crisis. With HIV and Ebola leaving deep scars in the history of these communities, stigma and broad fear of sickness challenged our response to the pandemic.
In Peru, it resulted in the death of a five-year-old girl of diphtheria—a disease preventable by an accessible vaccination. In Haiti, we saw hostility towards contact tracing and parents unwilling to bring their children to the hospital for fear of retribution from neighbors. CMMB-supported community health care workers were at the center of our response to this challenge, continuing to educate families on the importance of vaccinations, antenatal care, and seeking skilled deliveries—all the while debunking false information surrounding the virus and providing important prevention messaging to slow the spread.
3. Preexisting vulnerabilities compound suffering.

The pandemic has laid bare political, economic, and security vulnerabilities, especially in low income nations. In South Sudan, where health systems are starved of investment and communication infrastructure is almost non-existent, what little economic activity preexisted COVID-19 screeched to a halt. This reality posed challenges for keeping frontline workers and patients safe, in addition to limiting the dissemination of critical information about the virus and its spread.
Our response in the countries we serve, included improving technical infrastructure so CMMB field staff could work remote when possible, launching creative ways to share information safely and effectively within the communities, and mobilizing resources, like PPE and sanitation stations, to prepare under resourced health facilities for possible surges.
4. There’s another crisis looming and it’s not a virus.
The pandemic disrupted commercial supply chains and closed markets all over the world. But in places where food was already scarce, the pandemic is mounting the next global crisis—hunger.
Families have been forced to rely on the poor harvests produced by local farms. The story is the same in many of the world’s most impoverished countries. The World Food Program estimates 138 million people will require food assistance this year—the greatest need they’ve faced in six decades.
CMMB’s response includes the distribution of food items like maize flour, dried beans, cooking oil, baby formula and other essentials. In addition, we continue working with our partners on the ground to strengthen ongoing nutrition projects and programs.
5. There’s an unseen impact on our youth.
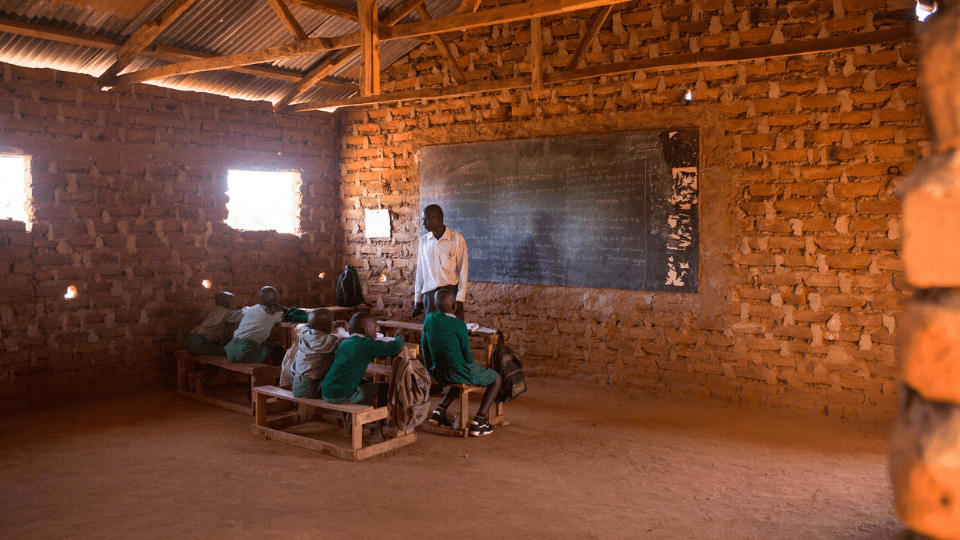
In countries like the United States, we saw the strain COVID-19 had on the education system. In places like Kenya or Zambia, where education may sometimes be sacrificed for families struggling to put food on the table, school closures and restrictions on attendance prolong the cycle of poverty.
It also increases the risk of teen pregnancy and drug and alcohol abuse among young people who are no longer receiving the sensitization messaging provided at school. CMMB’s country director in Kenya, Dr. James Kisia fears, “We may have lost a generation,” due to the secondary effects of COVID-19.
CMMB’s response includes the development of proper sanitation facilities at schools to help reduce the risk of spread while learning. In Kenya, for example, CMMB provided eight water tanks to vulnerable schools. In Zambia, our CHAMPS coordinator, Mwauluka is working with community leaders to develop a recreation center for youth to safely receive sensitization information when they aren’t, or can’t, be in the classroom.
6. In an emergency response, flexibility matters.
CMMB provides lifesaving services to women and children. At the onset of COVID-19 we worked quickly to reimagine our programs, like our First 100 Days Program in Peru or our cervical cancer initiatives in Kenya, to continue reaching women and children and widen our scope to include COVID-19 prevention efforts.
Both of these programs save lives in the communities they serve, and both of these programs can’t be put on pause—even in the face of a global pandemic.
7. Where there is crisis there is opportunity.
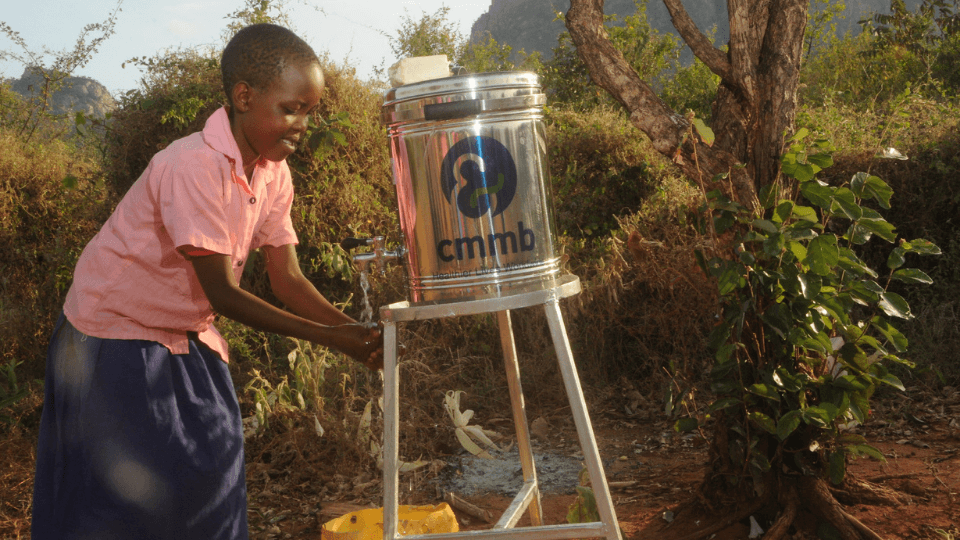
We knew from the beginning just how critical sanitation measures would be in the fight to save lives. That’s a challenging reality knowing that 3 billion people around the world lack access to basic sanitation and clean water. But with every crisis comes an opportunity and at CMMB, we seized it.
With the support of donors and the guidance of our staff on the ground, we launched multi-level initiative to help bring safe water, sanitation, and hygiene to vulnerable communities. Over the course of the pandemic we provided more than 100 handwashing stations and soap to health care facilities. In addition, we’ve trained thousands of community health workers to sensitize communities on the importance of handwashing for infection prevention.
Now, we are also running a student-led campaign, ACT4Water, to raise awareness about the global water crisis.
8. Women are our leaders on the frontlines.
Community health workers have been critical to our emergency response. Since before the onset of COVID-19, they have been essential to the provision of life-saving interventions such as childhood immunizations, reaching women for safe pregnancies, and more.
When the pandemic reached the communities they served, their roles became that much more important. In addition, adopting new, safe methods to relay information about these ongoing interventions, their work expanded to include education on COVID-19 and prevention. And leading this force of community health workers are women. From Haiti and Peru to Kenya, South Sudan, and Zambia, the vast majority of community health workers are women.
9. Our response will outlive the crisis.

The trainings we implement, the sanitation stations we build, the water tanks we place are evidence of long term change. While all these resources were implemented as part of our emergency response, their positive impact will last long after the pandemic is finally over. We’re building healthy habits and expanding access to resources that every child and mother deserves, regardless of the state of our world.
10. We can’t do it alone.
While we mourn the lives lost to COVID-19, we remain grateful for the lives we saved. But we didn’t save them alone. Our success is thanks to the support and dedication of people from all corners of the world, united by a mission to serve. Thanks to the bravery of our frontline health workers, the commitment of our country officers, and the compassion of our partners and donors, we launched a rapid, emergency response that is saving lives today—and for generations to come.